|
The following CBME core competencies are covered in this chapter.
|
Anatomy of Temporal Bone.
Introduction
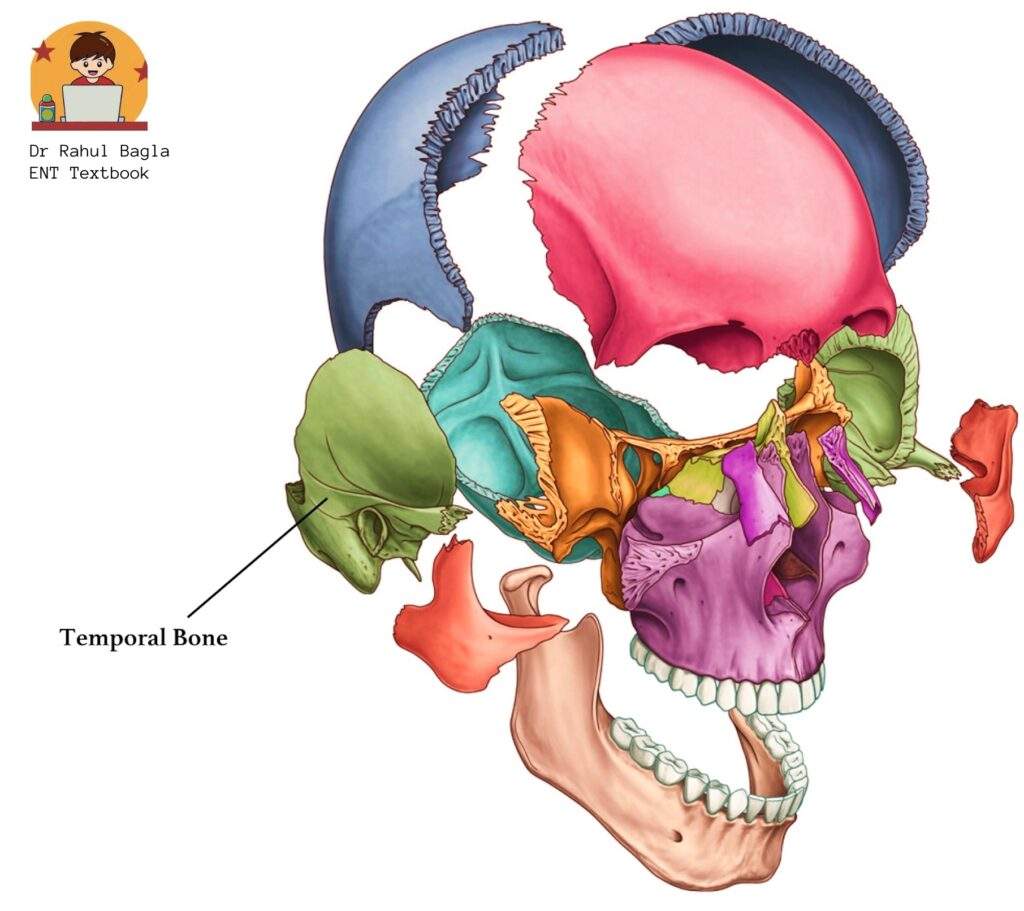
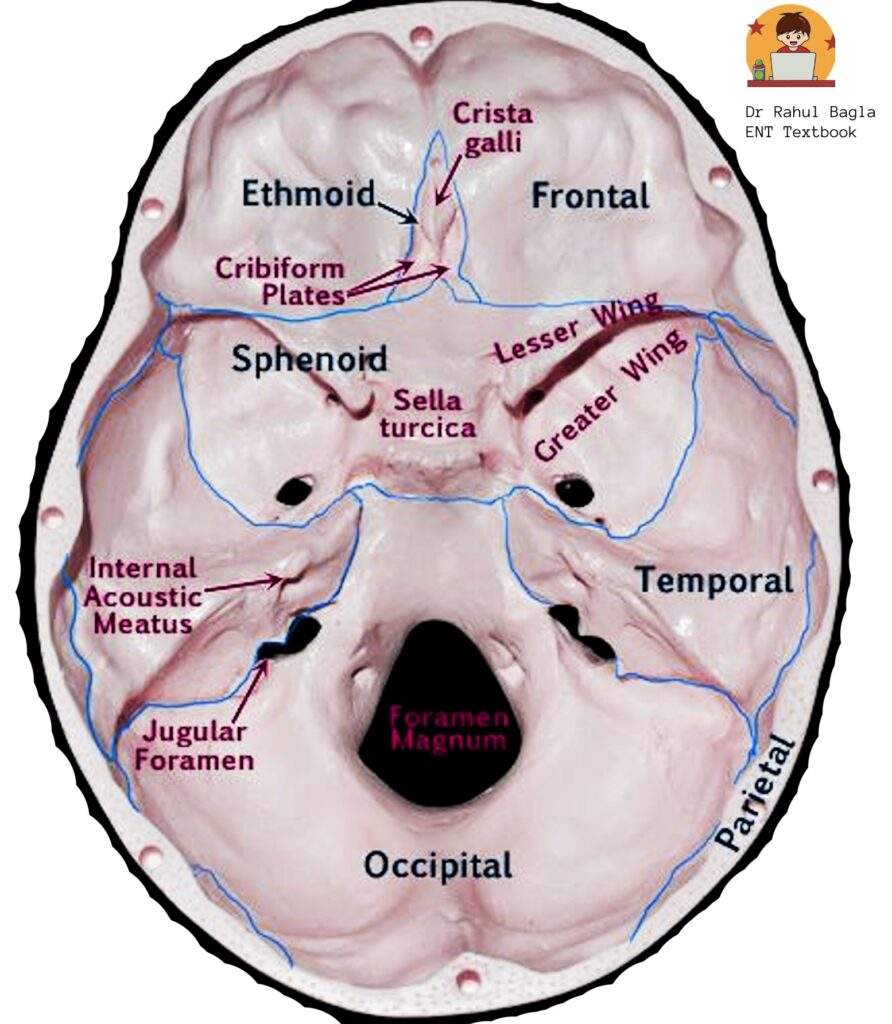
The temporal bone is a paired, symmetrical bone forming the lower lateral walls of the human skull. The temporal bone houses critical structures of the vestibulocochlear apparatus, including the external auditory canal, the middle ear and the inner ear. These components play essential roles in hearing and balance. The temporal bone also contributes to the formation of the middle cranial fossae, posterior cranial fossae and the overall base of the skull.
Relationships with Adjacent Bones
The temporal bone articulates with several other cranial bones:
- Anterior: The sphenoid bone lies anterior and medial to the temporal bone, with its greater wing articulating with the squamous part.
- Posterior: There is occipital bone.
- Inferior: The temporal bone articulates with the mandible, forming the temporomandibular joint, a synovial joint that facilitates jaw movement.
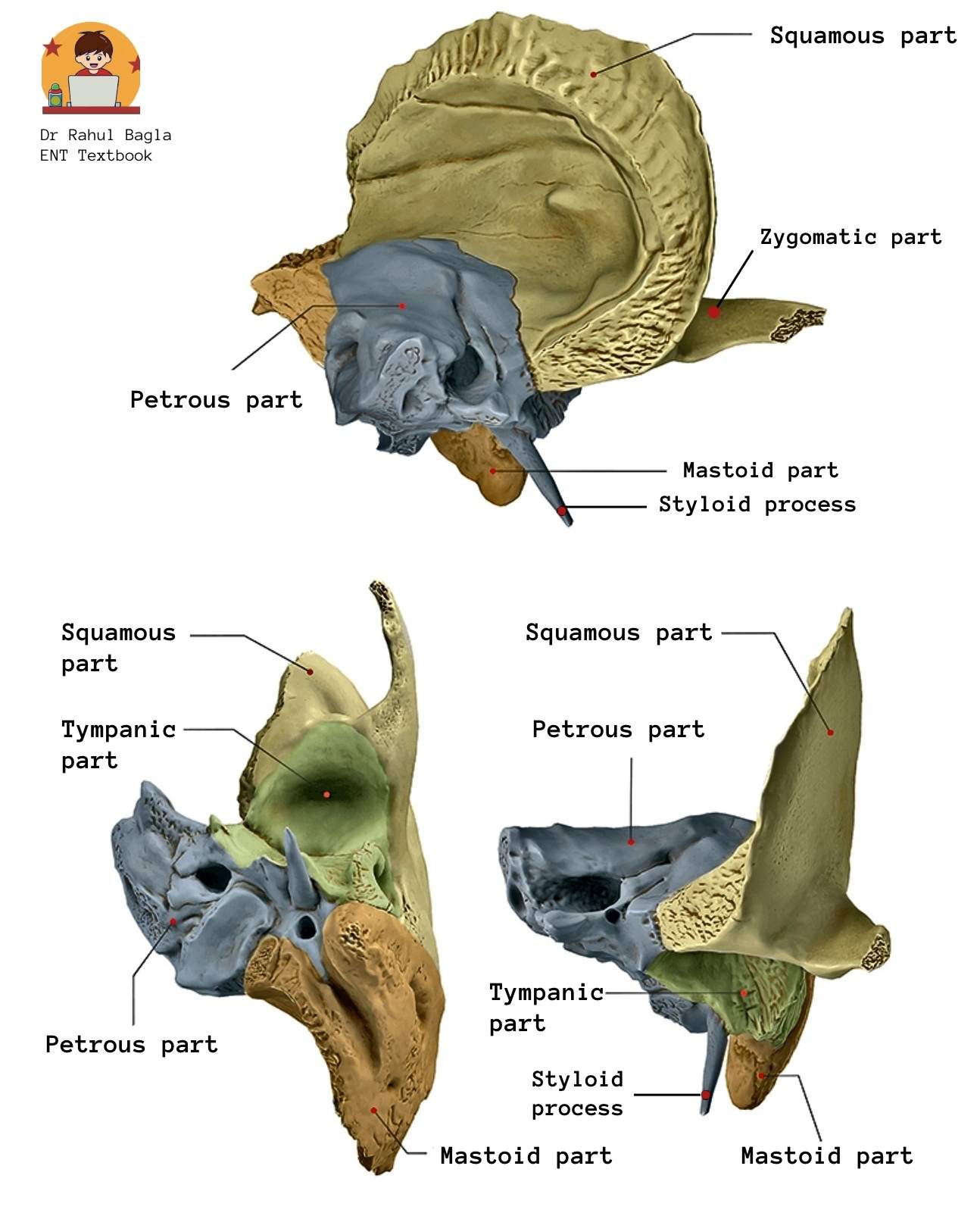
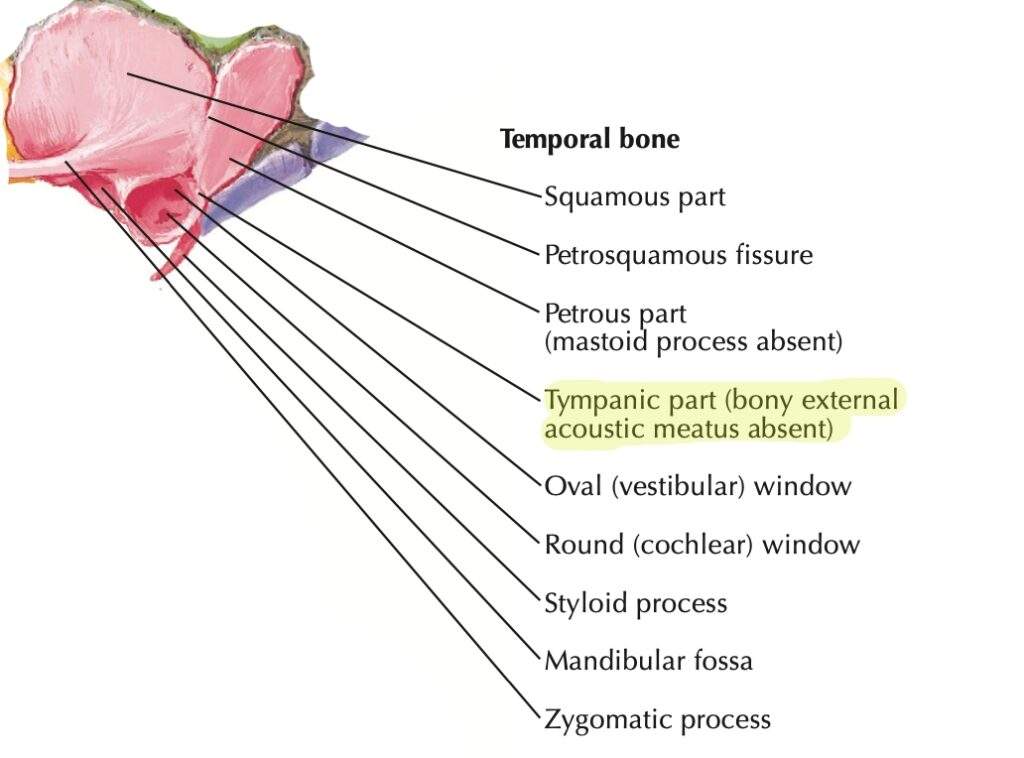
Parts of the temporal bone.
It is a composite structure consisting of five parts, each of which ossifies independently and later fuses during development.
-
Squamous: The largest and most superior part.
-
Petrous: The dense, pyramid-shaped part housing the inner ear.
-
Mastoid: The posterior, conically shaped part containing air cells.
-
Tympanic: Forms a significant portion of the external auditory canal.
-
Styloid: A slender, pointed projection.
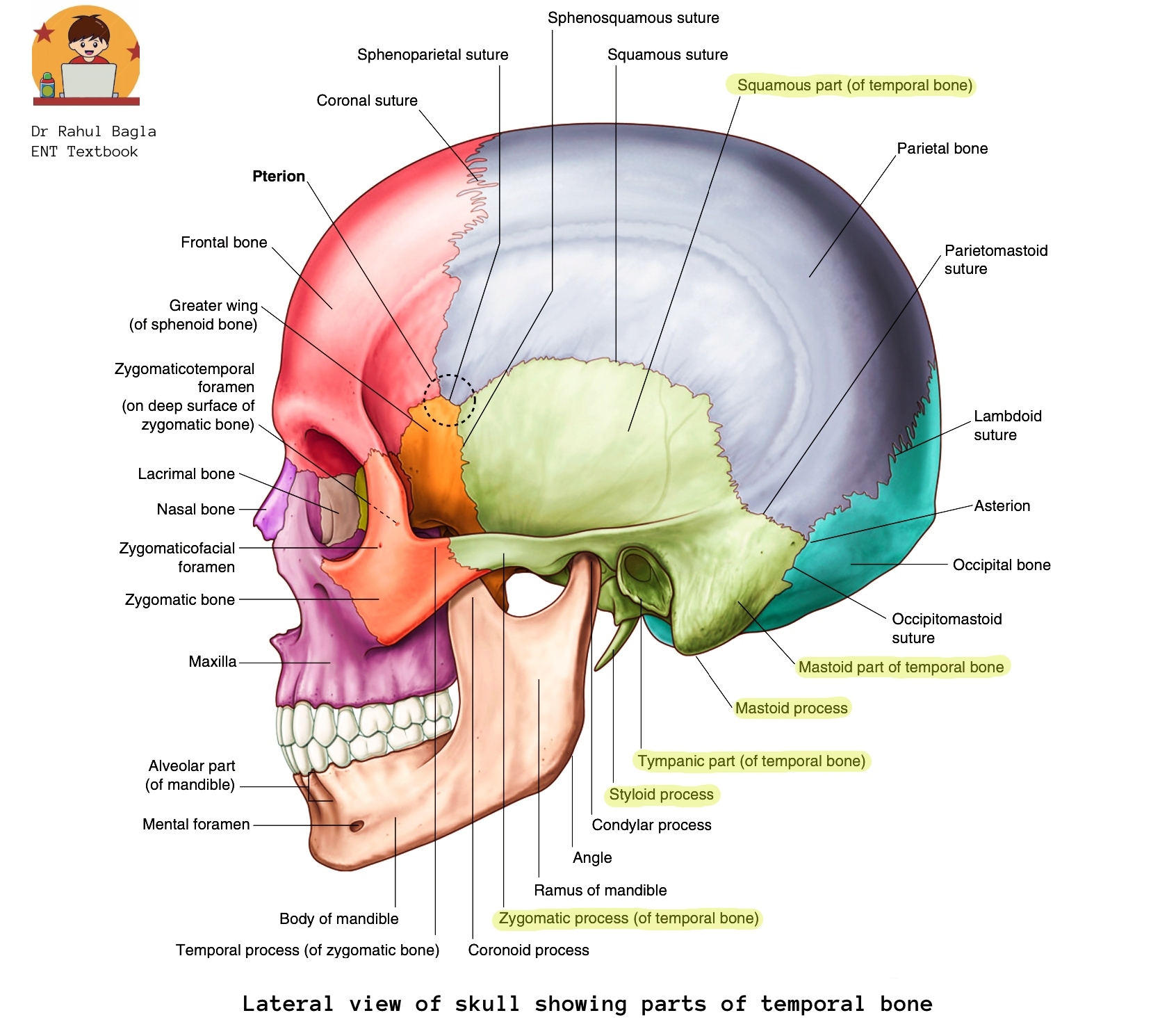

Squamous part of the temporal bone.
Squamous part (Squama). It is the largest and superior part of the temporal bone. It forms the lateral wall of the middle cranial fossa. It is a thin, translucent, shell-like plate of bone.
Relations:
- Superiorly: It interfaces with the parietal bone.
- Posteriorly: It connects with the mastoid part of the temporal bone.
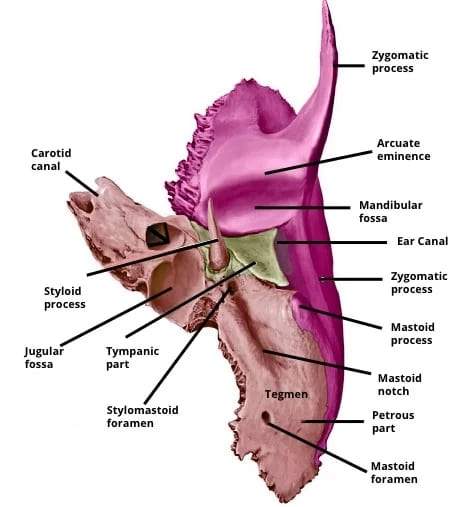
- Anteriorly: It articulates with the greater wing of the sphenoid bone and also gives rise to the zygomatic process, which articulates with the zygomatic bone to form the zygomatic arch, commonly palpable as the ‘cheekbone’.
- Mandibular fossa: The mandibular fossa is a depression that houses the synovial temporomandibular joint, and it lies below the zygomatic process.
- External Auditory Canal Formation: The squamous part primarily forms the roof of the external auditory canal (EAC), as well as small portions of the anterior and posterior walls. Whereas, the tympanic part of the temporal bone forms the rest of the EAC (a major part of the anterior and posterior walls, along with the inferior wall (floor) of the EAC).
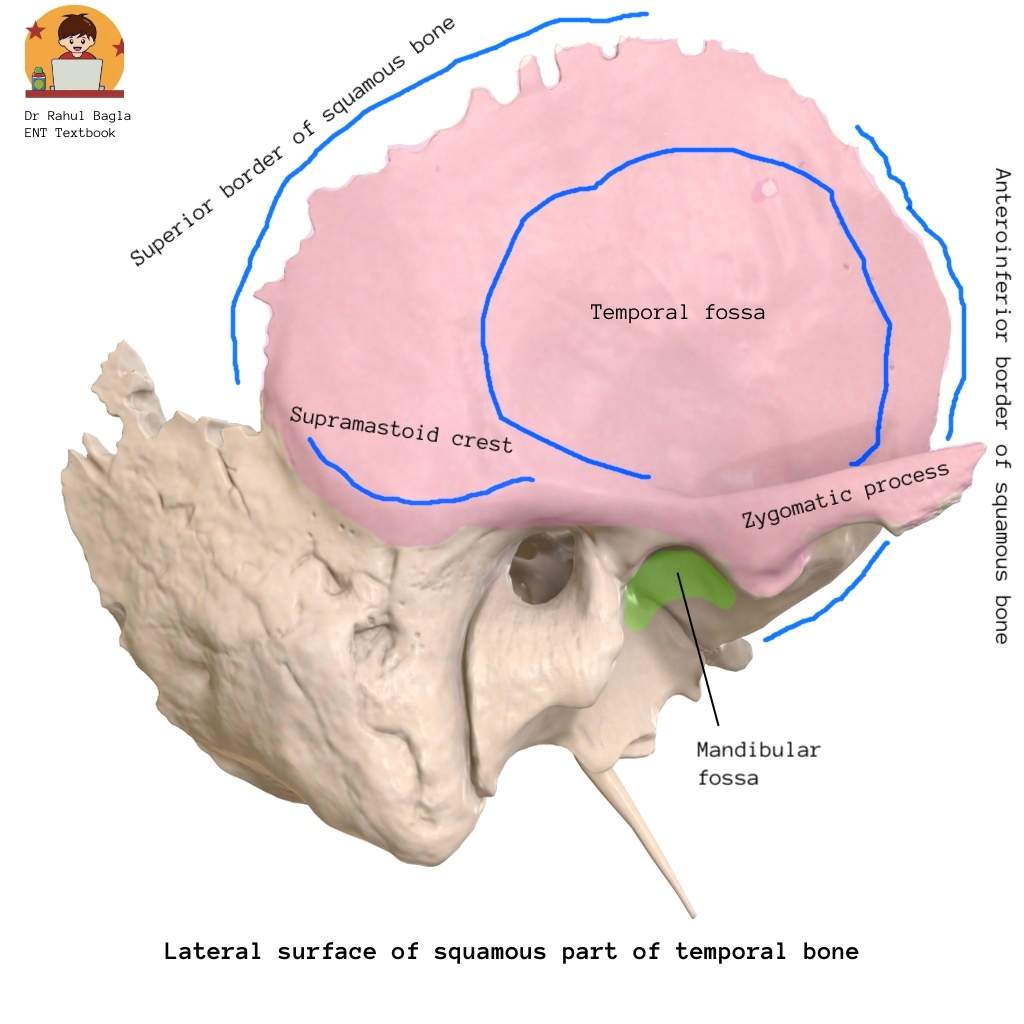
Surfaces and Borders of the Squamous Temporal Bone: The squamous part of the temporal bone has two surfaces (lateral and medial), two borders (superior and anteroinferior), a zygomatic process, and a mandibular fossa.
- Lateral surface (outer surface/ norma lateralis): It is convex in shape and forms the temporal fossa. The temporalis muscle originates from here. The lateral surface is limited posteriorly by the supramastoid crest, which provides attachment to the temporalis fascia. The squamous part is separated from the mastoid part by an imaginary suture line, which gets fused about 1.5 cm posterior to the supramastoid crest. On the lateral surface, the middle temporal artery runs in a groove. The zygomatic process projects from the lateral surface of the squamous part of the temporal surface, which articulates with the zygomatic bone to form the zygomatic arch, commonly palpable as the ‘cheekbone’.
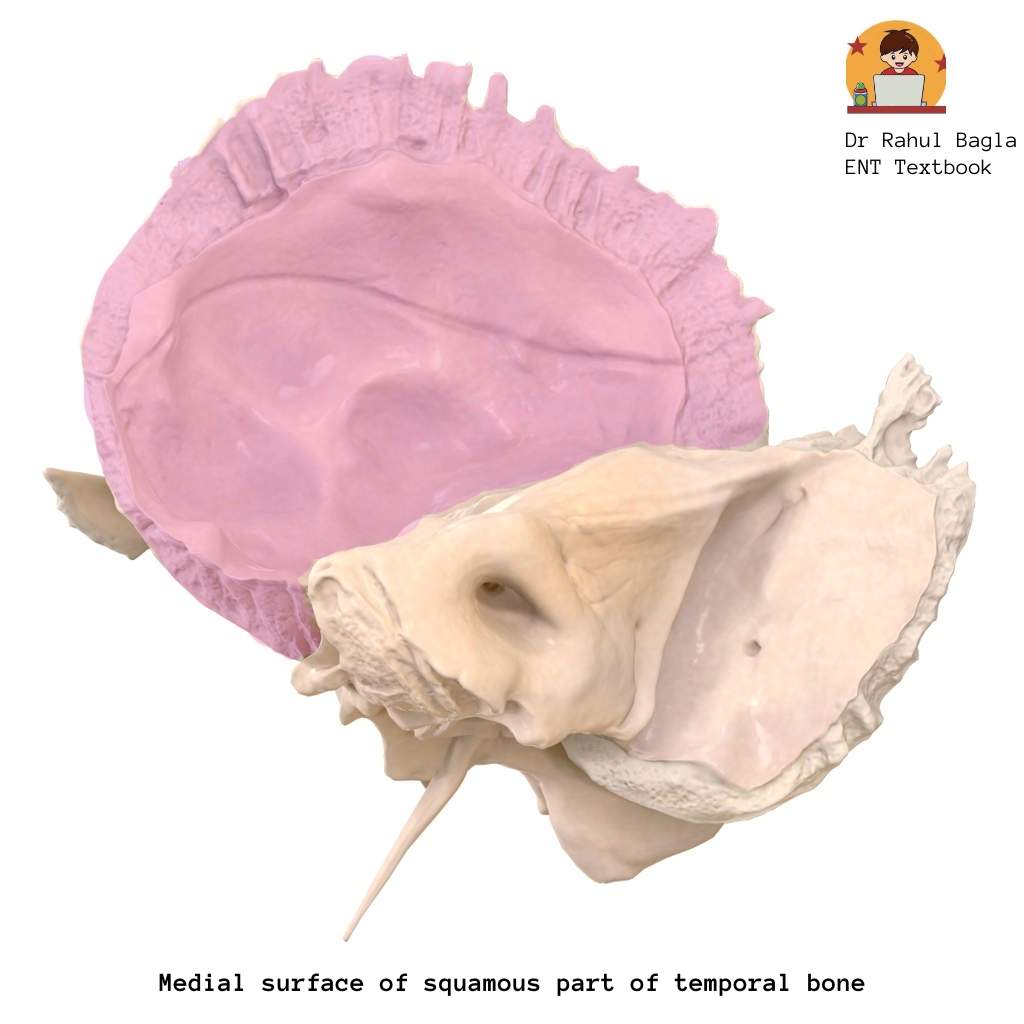
- Medial surface (inner/cerebral surface): It is related to the temporal lobe of the brain. Anterior and posterior branches of the middle meningeal artery run over this surface, making it clinically significant in trauma.
- Superior border: It articulates with the inferior border of the parietal skull bone, forming part of the coronal suture.
- Anteroinferior border: It articulates with the greater wing of the sphenoid bone. It forms the posterolateral aspect of the infratemporal fossa.
Clinical Correlate (Important): The greater wing of the sphenoid, parietal and frontal bones together with the squamous part of the temporal bone form the pterion, which is the weakest part of the skull. Trauma to the pterion can lead to significant intracranial haemorrhage, particularly an epidural hematoma due to injury to the middle meningeal artery, which lies beneath it.
Tympanic part of the temporal bone.
The tympanic part is situated lateral to the petrous part of the temporal bone, inferiorly to the squamous part of the temporal bone, and anteriorly to the mastoid part of the temporal bone. The tympanic part is attached to the squamous part and mastoid part, forming the tympanosquamous anteriorly and tympanomastoid sutures posteriorly. It is a triangular bony plate. It has three borders (superior, inferior & lateral) and two surfaces (anterior & posterior):
Relations of the tympanic part of the temporal bone:
-
Superior border is related to the mandibular fossa.
-
Inferior border is related to the styloid process and the inferior aspect of the petrous part of the temporal bone.
-
Lateral border, along with the posterior surface, forms the anterior wall, the floor and the lower part of the posterior wall of the bony ear canal. The tympanic bone boundary ends at the cartilaginous EAC.
-
Anterior surface is related to the parotid gland & mandibular fossa.
-
Posterior surface, it bears a circular groove, the tympanic sulcus (annular sulcus) for the attachment of the tympanic membrane.
Important Structures Related to the Tympanic Part
Chorda tympani, anterior tympanic artery and anterior process of malleus traverse the petrotympanic fissure. Arnold’s nerve traverses the tympanomastoid suture. The inferior aspect of the tympanomastoid suture line is an important operative landmark for identifying the facial nerve as it exits the stylomastoid foramen.
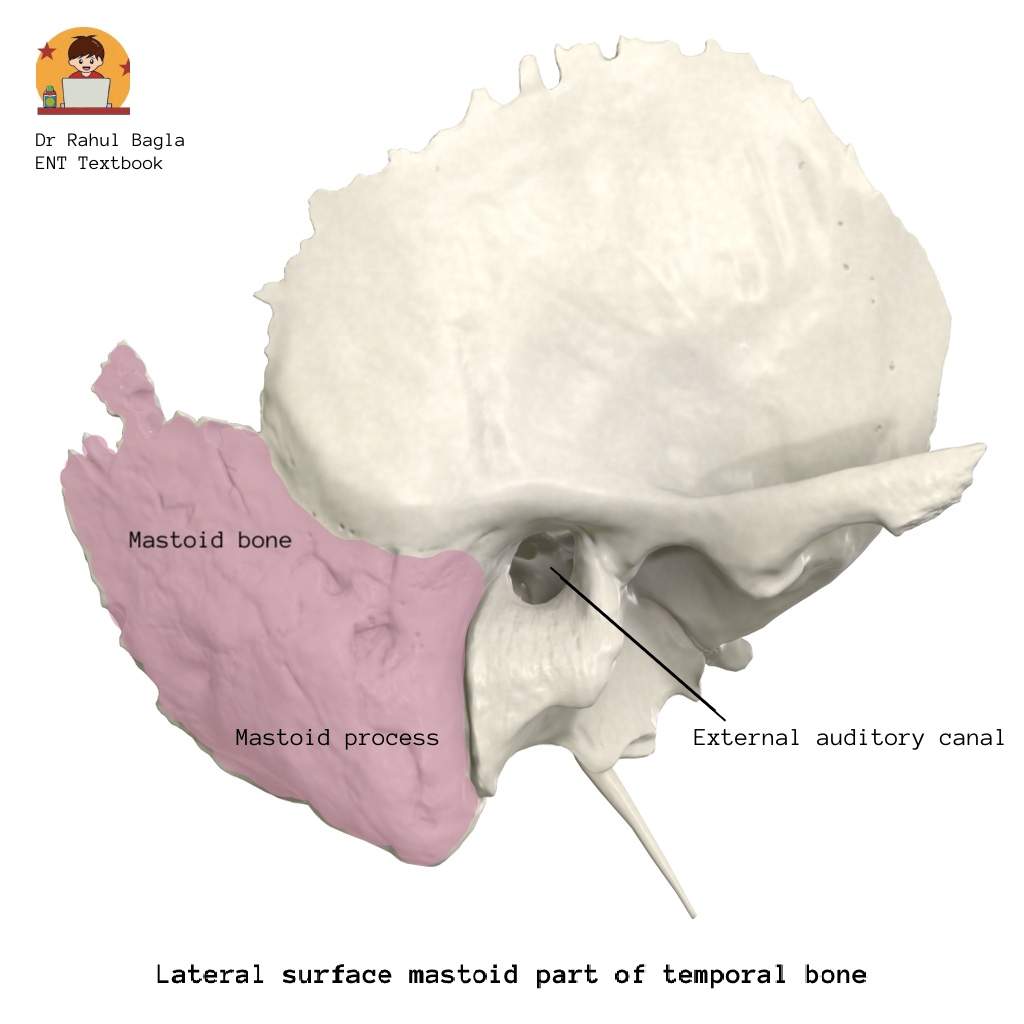
Mastoid part of the temporal bone.
It is situated posterior to the squamous part of the temporal bone and separates from it by an imaginary suture line, which gets fused about 1.5 cm posterior to the supra-mastoid crest. The mastoid part of the temporal bone includes the mastoid antrum and its air cells, which communicate with the middle ear cavity. It is formed by the squamous part of the temporal bone (laterally) and the petrous part of the temporal bone (medially), separated by Korner’s (petrosquamous) septum. It has two surfaces (lateral and medial) and two borders (superior and posterior).
Surfaces of the Mastoid Part
-
Lateral surface is continuous with the mastoid process, which provides attachment of the sternocleidomastoid, splenius capitis and longissimus capitis muscles. The mastoid process is present just posterior to the external auditory canal opening, and it is not fully developed in children. A more horizontal postauricular incision should be given to prevent injury to the facial nerve.
-
Medial/ inner surface of the mastoid part of the temporal bone forms the sigmoid sulcus, which lodges the sigmoid sinus. The medial surface is further continuous with the posterior surface of the petrous part of the temporal bone. The medial surface of the mastoid process, which is present inferior to the mastoid part of the temporal bone, presents a digastric notch that presents attachment to the posterior belly of the digastric muscle. The groove for the occipital artery lies medial to the digastric notch. The mastoid foramen is also present on the medial surface of the mastoid process, through which passes the mastoid emissary vein for venous drainage and one or two mastoid arteries.
Borders of the Mastoid Part
-
Superior border articulates with the inferior border of the parietal bone, forming the parietomastoid suture.
-
Posterior border articulates with the occipital bone, forming the occipitomastoid suture.
Clinical Landmark: The mastoid part of the temporal bone, parietal and occipital bones meet at a point to form the asterion.
Medial and Inferior surface of mastoid part of temporal bone
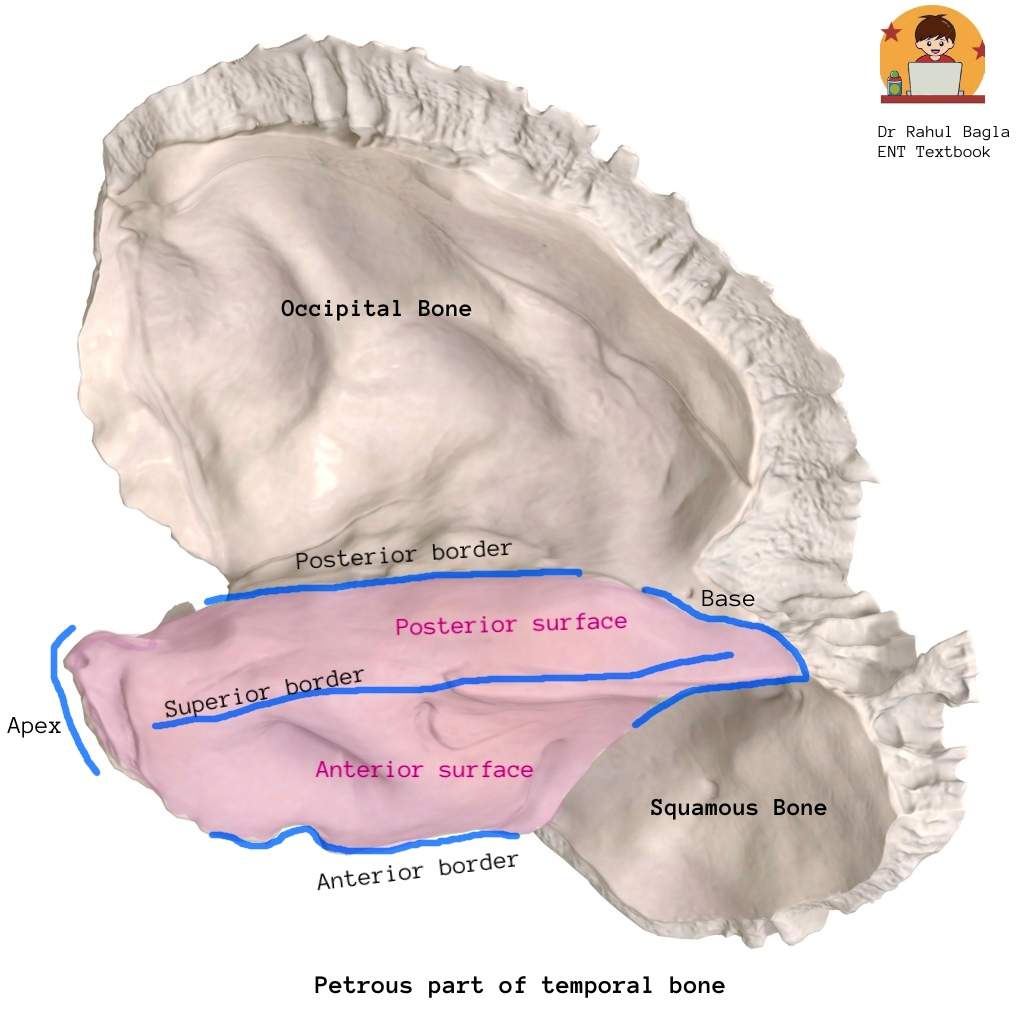
Petrous part of the temporal bone.
Petrous (rock-like) part: It is located within the base of the skull, positioned between the greater wing of the sphenoid bone anteriorly and the occipital bone posteriorly. It houses the middle ear, internal ear and mastoid antrum, which it safely shields due to its high bone density. It separates the middle cranial fossa from the posterior cranial fossa and it also forms a part of the cranial floor.
General Features and Relations of the Petrous Part
It is a pyramid-shaped structure, having a base, an apex, three surfaces (anterior, posterior, inferior) and three edges or margins (superior, anterior, posterior).
-
Base: It is fused with the medial surface of the squamous part of the temporal bone and with the medial surface of the mastoid part of the temporal bone.
-
Apex: It is directed forwards, upwards, medially towards the greater wing and the body of the sphenoid bone. At the petrous apex, the trigeminal nerve (CN V) enters Meckel’s cave. The abducens nerve (CN VI) passes close to its roof within Dorello’s canal.
Clinical correlate: Gradenigo’s syndrome occurs due to infection at the petrous apex and comprises retroorbital pain (Vth nerve involvement), lateral rectus palsy, diplopia (VIth nerve involvement), and a discharging ear from middle ear infection.
Apex forms the posterolateral margin of the foramen lacerum. Apex also presents an internal opening of the carotid canal, which carries the petrous part of the internal carotid artery. The apex and the sphenoid bone, together with the basilar part of the occipital bone, make a lacerated foramen at the meeting point known as the foramen lacerum.

Surfaces of the Petrous Part
-
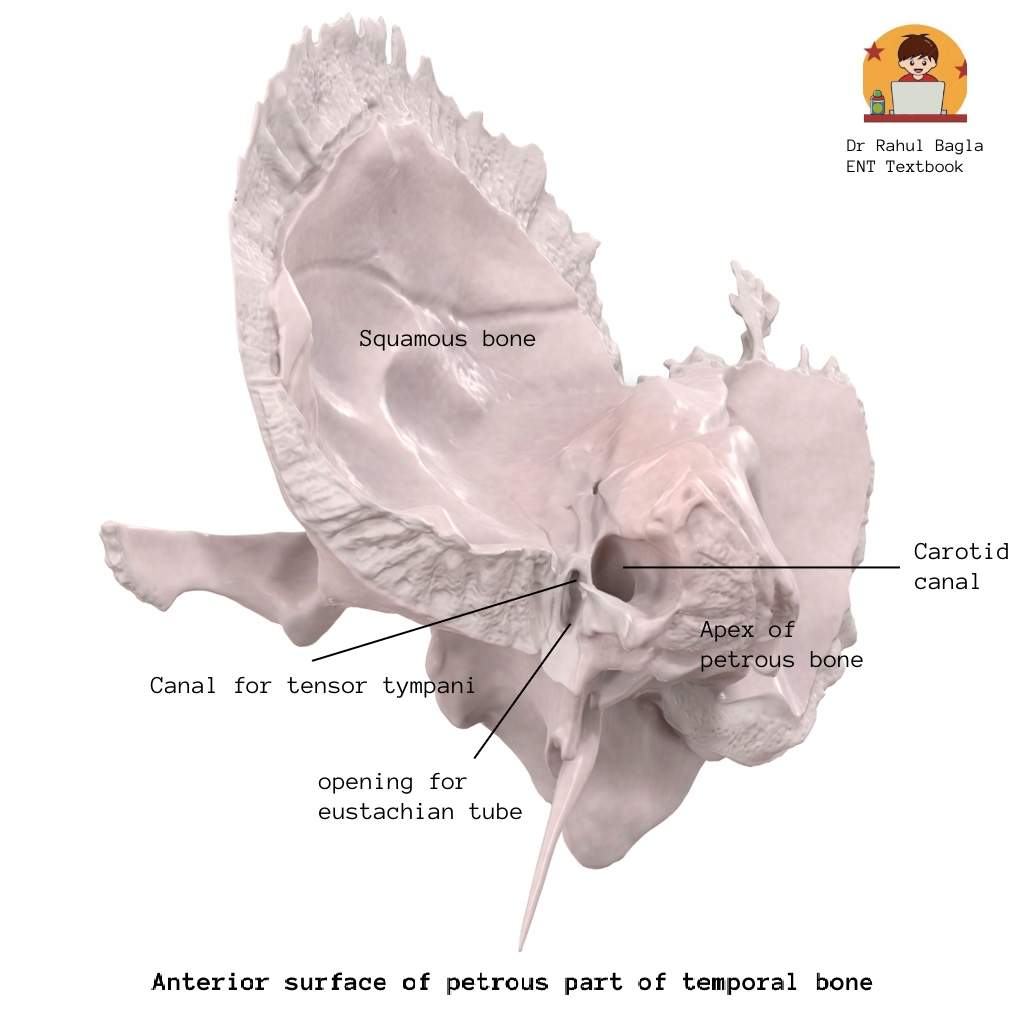
Anterior surface: It forms the posterior wall of the middle cranial fossa. It presents four important structures (medial to lateral): the trigeminal impression (lodges the trigeminal ganglion), the roof of the internal acoustic meatus, the arcuate eminence and the roof of the middle ear (tegmen tympani).
The depressed area, just lateral to the trigeminal impression, is the roof of the internal acoustic meatus. The elevated area, just lateral to the roof of the internal acoustic meatus, is the arcuate eminence, which is formed by the underlying superior semicircular canal.
The rest of the area lateral to the arcuate eminence towards the squamous part of the temporal bone is the roof of the middle ear (tegmen tympani). The area of the roof of the middle ear cavity presents two hiatus for the greater and lesser petrosal nerves. It also presents two openings, the canal for tensor tympani (upper one) and the opening of the bony part of the eustachian tube (lower one), both of which open in the middle ear cavity. -
Posterior surface: It forms the anterior wall of the posterior cranial fossa. It presents an important structure, the opening of the internal acoustic meatus. The internal acoustic meatus is one cm in length, and it is in line with the external auditory canal.
The vestibulocochlear nerve, facial nerve and labyrinthine artery enter from the medial opening of the internal acoustic meatus (also known as porus) and pass through it. At the lateral opening of the internal acoustic meatus (also known as fundus), the meatus is divided into upper and lower compartments by a bony plate, the ‘horizontal crest’.
On the anterior aspect of the upper compartment, there is a facial canal through which the facial nerve passes, and on the posterior aspect, there is the superior vestibular area through which the superior division of the vestibular nerve passes.
On the anterior aspect of lower compartment, there are spiral-shaped multiple foramina (known as tractus spiralis foraminosus) through which the cochlear nerve passes, and on the posterior aspect, there is the inferior vestibular area through which the inferior division of the vestibular nerve passes. On the most posterior aspect of the lower compartment, there is also a foramen singulare through which the branch of the vestibular nerve passes, which supplies the ampulla of the posterior semicircular canal.
-
Inferior surface: It is a quadrangular area viewed in the base of the skull. It is located between the occipital bone posteriorly and the greater wing of the sphenoid & squamous part anteriorly. The inferior surface presents the outer opening of the carotid canal. Lateral to the carotid canal lies the jugular fossa. The stylomastoid foramen is also present on the inferior surface through which the facial nerve exits from the middle ear.
Borders (Margins) of Petrous Part
-
Superior border: It is a long, sharp crest that intervenes between the middle and posterior cranial fossae. It provides attachment to the tentorium cerebelli, and it encloses the superior petrosal sinus.
-
Anterior border: It can be divided into two parts. The medial part articulates with the greater wing of the sphenoid, while the lateral part joins with the squamous part of the temporal bone with a suture – petrosquamosal suture.
-
Posterior border: It presents a groove that lodges the inferior petrosal sinus. Its lateral part creates the superolateral boundary of the jugular foramen.
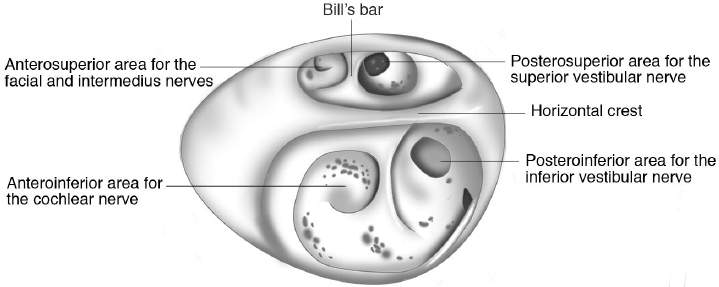
Lateral end of the internal acoustic meatus (Fundus)
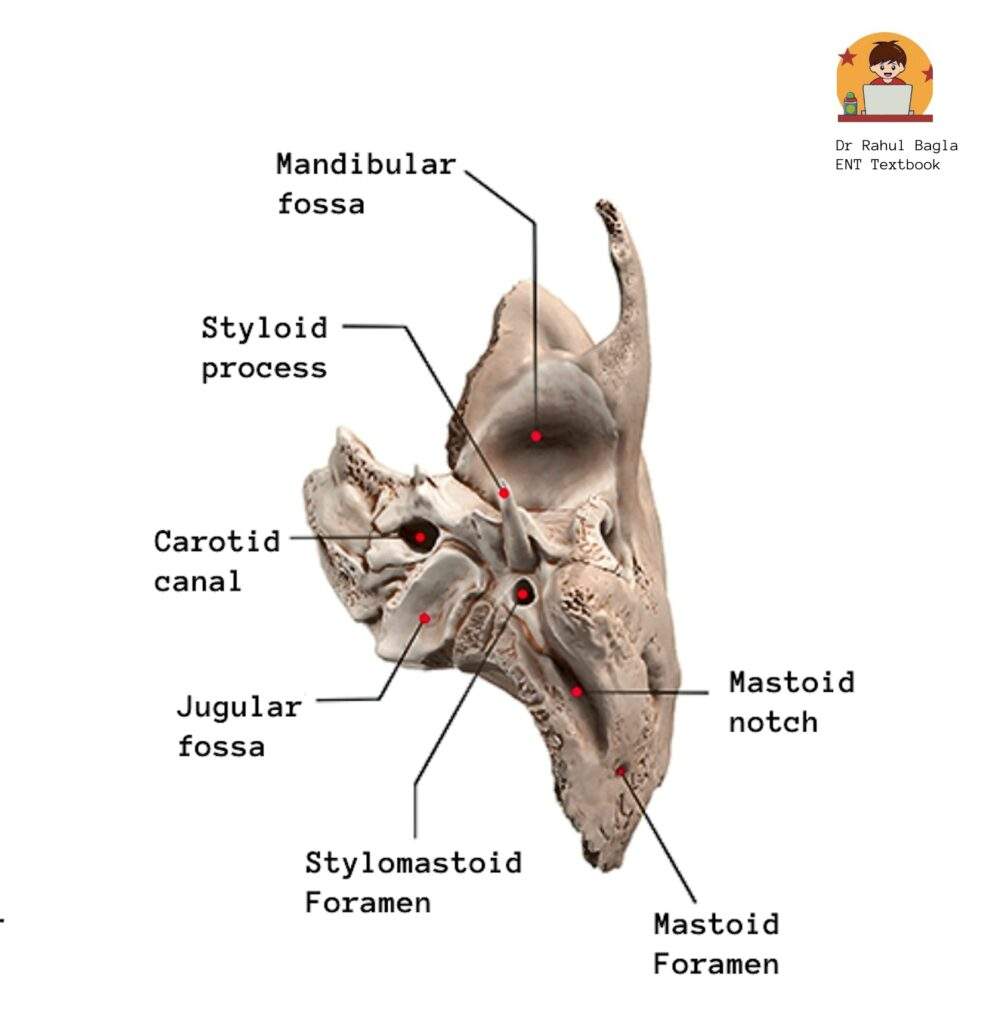
Inferior surface of the petrous part of the temporal bone
Styloid part of the temporal bone.
The styloid process is a long, slender, pointed piece of bone originating from the inferior aspect of the fusion of the tympanic and petrous bones and located in front of the jugular fossa. Its normal length is approximately 2.5 cm. It projects downwards, forwards and medially, giving attachment to several muscles and ligaments.
Attachments of the Styloid Process
-
Ligaments – Stylohyoid, stylomandibular
-
Muscles – Styloglossus, stylohyoid, stylopharyngeus.
Styloglossus is supplied by the hypoglossal nerve, stylohyoid is supplied by the facial nerve, and stylopharyngeus is supplied by the glossopharyngeal nerve.
Stylomandibular Ligament: The stylomandibular ligament extends from the anterior surface of the apex of the styloid process to the posterior surface of the angle of the mandible. This ligament separates the parotid gland from the submandibular gland & medial pterygoid muscle.
Stylomastoid Foramen (Important): The stylomastoid foramen is a round opening situated between the styloid and the mastoid processes. It transmits the facial nerve (CN VII) and the stylomastoid artery.
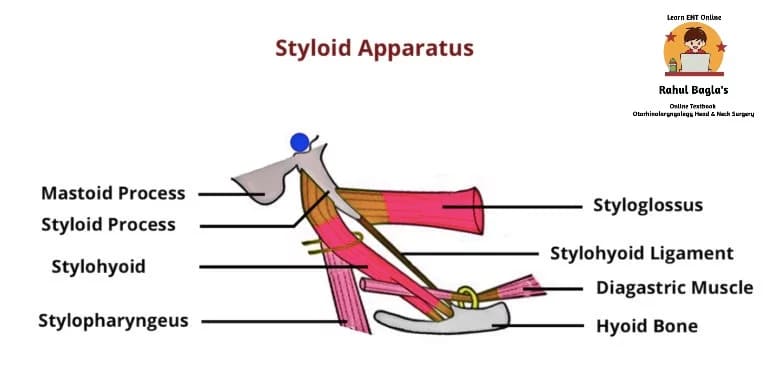
Table: Parts of the Temporal Bone
| Part of Temporal Bone | Location / Description | Major Structures / Contribution | High-Yield Clinical Importance |
| Squamous Part | Largest, superior part; thin shell-like plate | Forms lateral wall of middle cranial fossa, gives zygomatic process, forms roof of EAC partly | Pterion area related to middle meningeal artery → epidural hematoma |
| Tympanic Part | Inferior to squamous, lateral to petrous, anterior to mastoid | Forms major part of bony EAC, has tympanic sulcus for TM attachment | Petrotympanic fissure → chorda tympani passes |
| Mastoid Part | Posterior to squamous | Contains mastoid antrum + air cells, related to sigmoid sinus | Mastoid surgery landmark: sigmoid sinus, facial nerve risk in children |
| Petrous Part | Dense pyramid inside skull base | Houses middle ear, inner ear, ICA canal, IAC | Petrous apex infection → Gradenigo syndrome |
| Styloid Part | Slender downward projection | Muscle + ligament attachments | Stylomastoid foramen transmits facial nerve |
———— End of the chapter ————
High-Yield Points for NEET PG and University Exams
- Weakest part of skull: Pterion (formed by temporal squamous, parietal, frontal, and sphenoid greater wing). Damage here risks middle meningeal artery injury.
- Temporal bone parts: Squamous, Petrous, Mastoid, Tympanic, Styloid.
- Petrous Apex Syndrome (Gradenigo’s): Retro-orbital pain (V), Lateral rectus palsy (VI), Discharging ear.
- Arcuate Eminence: Formed by superior semicircular canal, important surgical landmark.
- Tegmen Tympani: Roof of middle ear cavity.
- Internal Acoustic Meatus (IAM) Contents: Facial nerve (CN VII), Vestibulocochlear nerve (CN VIII), Labyrinthine artery.
- Horizontal Crest (Falciform Crest): Divides IAM fundus into superior (Facial, Superior Vestibular) and inferior (Cochlear, Inferior Vestibular) compartments.
- Stylomastoid Foramen: Exit point for Facial Nerve (CN VII) and Stylomastoid artery. Key landmark for facial nerve identification.
- Tympanomastoid Suture: Landmark for facial nerve identification inferiorly. Traversed by Arnold’s nerve (auricular branch of vagus).
- Petrotympanic Fissure (Glaserian Fissure): Transmits chorda tympani, anterior tympanic artery, anterior malleolar process.
- Styloid Muscles innervation: Stylohyoid (Facial), Styloglossus (Hypoglossal), Stylopharyngeus (Glossopharyngeal). (Mnemonic: FGH for Good Health).
- Mastoid process in children: Undeveloped, facial nerve more superficial, hence risk of injury with vertical incisions.
- Sigmoid Sulcus: Lodges Sigmoid Sinus. Mastoid infections can spread here.
MCQ’s – For NEET PG and University Exams
Instructions: Choose the single best answer for each question.
- Which of the following bones does NOT contribute to the formation of the pterion? a) Frontal bone b) Parietal bone c) Occipital bone d) Squamous part of temporal bone e) Greater wing of sphenoid bone
- Gradenigo’s syndrome is characterized by the involvement of which two cranial nerves in addition to otorrhea? a) Trigeminal and Hypoglossal b) Facial and Vestibulocochlear c) Trigeminal and Abducent d) Glossopharyngeal and Vagus e) Oculomotor and Trochlear
- The arcuate eminence on the anterior surface of the petrous temporal bone is formed by the bulging of which structure? a) Cochlea b) Posterior semicircular canal c) Superior semicircular canal d) Vestibule e) Facial nerve canal
- Which of the following structures exits the skull through the stylomastoid foramen? a) Vestibulocochlear nerve b) Chorda tympani nerve c) Greater petrosal nerve d) Facial nerve e) Lingual nerve
- The tympanic sulcus, located on the posterior surface of the tympanic part of the temporal bone, serves as the attachment point for which structure? a) Malleus b) Incus c) Stapes d) Tympanic membrane e) Eustachian tube
- Korner’s septum, if present, separates which two parts of the temporal bone within the mastoid? a) Squamous and Petrous b) Tympanic and Mastoid c) Squamous and Mastoid d) Petrous and Mastoid e) Tympanic and Petrous
- Which of the following ligaments is NOT attached to the styloid process? a) Stylohyoid ligament b) Stylomandibular ligament c) Sphenomandibular ligament d) All are attached to the styloid process
- The horizontal crest (falciform crest) divides the fundus of the internal acoustic meatus into upper and lower compartments. Which nerve passes through the anterior aspect of the upper compartment? a) Superior vestibular nerve b) Cochlear nerve c) Facial nerve d) Inferior vestibular nerve e) Glossopharyngeal nerve
- Which anatomical landmark is critical for identifying the facial nerve during mastoid surgery, especially its exit point? a) Arcuate eminence b) Tegmen tympani c) Tympanic sulcus d) Inferior aspect of the tympanomastoid suture line e) Digastric notch
- The sigmoid sulcus on the medial surface of the mastoid part of the temporal bone lodges which important venous structure? a) Cavernous sinus b) Inferior petrosal sinus c) Superior petrosal sinus d) Sigmoid sinus e) Transverse sinus
Answers: 1: C 2: C 3: C 4: D 5: D 6: A 7: C 8: C 9: D 10: D
Clinical Scenario Questions
Instructions: Analyse the following scenarios and answer the questions, considering the anatomical knowledge of the temporal bone.
1. Scenario: A 45-year-old male presents to the emergency department after a fall, sustaining a head injury. He has a hematoma over his left temple, and imaging reveals a skull fracture crossing the pterion. What is the most significant vascular structure at risk of injury in this specific region, and what type of intracranial haemorrhage would typically result? Answer: The most significant vascular structure at risk at the pterion is the middle meningeal artery. Injury to this artery typically results in an epidural hematoma, characterised by a lenticular (lens-shaped) collection of blood between the dura mater and the skull.
2. Scenario: A 7-year-old child presents with a history of chronic suppurative otitis media (CSOM) with a recent onset of severe retro-orbital pain, diplopia, and persistent purulent ear discharge. On examination, there is also a slight lateral gaze weakness. Based on the anatomical relations of the temporal bone, what is the likely diagnosis, and which specific part of the temporal bone is primarily involved? Answer: The likely diagnosis is Gradenigo’s Syndrome. This triad of symptoms (retro-orbital pain, diplopia/lateral gaze weakness, and discharging ear) points to an infection spreading to the petrous apex of the temporal bone, affecting the trigeminal (CN V) and abducent (CN VI) nerves, which are in close proximity.
3. Scenario: During a mastoidectomy procedure in an adult, the surgeon is attempting to identify the facial nerve’s exit point from the temporal bone. What specific anatomical landmark would the surgeon look for, particularly on the inferior aspect of the posterior ear canal, to safely locate this nerve? Answer: The surgeon would look for the tympanomastoid suture line, specifically its inferior aspect. This suture is a reliable external landmark, as the stylomastoid foramen, through which the facial nerve exits, is located just inferior to it.
4. Scenario: A patient develops Bell’s palsy, presenting with an acute onset unilateral facial weakness. Knowing the anatomical course of the facial nerve, what is the most likely segment of the nerve within the temporal bone to be affected in such cases, and which foramen does the nerve typically exit through to supply facial muscles? Answer: In cases of Bell’s palsy, the most likely segment of the facial nerve affected within the temporal bone is the intratemporal segment, particularly within the facial canal (also known as the Fallopian canal), often due to inflammation and oedema causing compression. The nerve exits the skull through the stylomastoid foramen to innervate the muscles of facial expression.
Frequently Asked Questions in Viva
- Q: What is the main function of the temporal bone? A: The temporal bone primarily houses and protects the critical structures involved in hearing and balance, including the middle ear, inner ear, and parts of the external ear.
- Q: Which part of the temporal bone forms the roof of the middle ear cavity? A: The tegmen tympani, which is a part of the petrous temporal bone, forms the roof of the middle ear cavity.
- Q: Why is the pterion clinically important? A: The pterion is clinically important because it is the weakest part of the skull, and trauma to this region can easily injure the underlying middle meningeal artery, leading to an epidural hematoma.
- Q: What structures pass through the Internal Acoustic Meatus (IAM)? A: The Internal Acoustic Meatus (IAM) transmits the facial nerve (CN VII), the vestibulocochlear nerve (CN VIII), and the labyrinthine artery.
- Q: How can a surgeon identify the facial nerve during mastoid surgery? A: Surgeons often identify the facial nerve by locating the inferior aspect of the tympanomastoid suture line and following it towards the stylomastoid foramen, which is the nerve’s exit point.
- Q: What is Gradenigo’s syndrome, and what causes it? A: Gradenigo’s syndrome is a triad of retro-orbital pain, lateral rectus palsy/diplopia, and persistent otorrhea, caused by the spread of middle ear infection to the petrous apex of the temporal bone.
- Q: Which muscles attach to the styloid process, and what are their innervations? A: The muscles attached to the styloid process are the styloglossus (CN XII), stylohyoid (CN VII), and stylopharyngeus (CN IX).
Reference Textbooks.
- Scott-Brown, Textbook of Otorhinolaryngology-Head and Neck Surgery.
- Glasscock-Shambaugh, Textbook of Surgery of the Ear.
- P L Dhingra, Textbook of Diseases of Ear, Nose and Throat.
- Hazarika P, Textbook of Ear Nose Throat And Head Neck Surgery Clinical Practical.
- Mohan Bansal, Textbook of Diseases of Ear, Nose and Throat Head and Neck Surgery
- Hans Behrbohm, Textbook of Ear, Nose, and Throat Diseases With Head and Neck Surgery.
- Salah Mansour, Middle Ear Diseases – Advances in Diagnosis and Management.
- Logan Turner, Textbook of Diseases of The Nose, Throat and Ear Head And Neck Surgery.
- Rob and smith, Textbook of Operative surgery.
- Anirban Biswas, Textbook of Clinical Audio-vestibulometry.
- Arnold, U. Ganzer, Textbook of Otorhinolaryngology, Head and Neck Surgery.
Author:

Dr. Rahul Bagla
MBBS (MAMC, Delhi) MS ENT (UCMS, Delhi)
Fellow Rhinoplasty & Facial Plastic Surgery.
Renowned Teaching Faculty
Mail: msrahulbagla@gmail.com
India
———– Follow us on social media ————
- Follow our Facebook page: https://www.facebook.com/Dr.Rahul.Bagla.UCMS
- Follow our Instagram page: https://www.instagram.com/dr.rahulbagla/
- Subscribe to our Youtube channel: https://www.youtube.com/@Drrahulbagla
- Please read. Anatomy of External Ear. https://www.entlecture.com/anatomy-of-ear/
- Please read. Anatomy of Temporal Bone. https://www.entlecture.com/anatomy-of-temporal-bone/
- Please read. Stenger’s, Chimani Moos, Teal test. https://www.entlecture.com/special-tuning-fork-tests/
Thank you Dr. Rahul, excellent job.
Very clear and engaging writing style. Thanks
Wonderful work. Your temporal bone content is easy to learn. Please upload PPT.
Selamlar from Ankara!”
Thank you so much
Regards
Dr Rahul
“As a PG student at Charité – Universitätsmedizin Berlin, Germany. I find this online resource incredibly helpful. The PDF links are top-notch. Thank you
Well explained